2022 Randomized Controlled Trial: Adipose Therapy Superior to PRP for Advanced Knee Osteoarthritis (OA)
When the Question Isn’t Whether to Try a Biologic — But Which One
Orthobiologics represent a significant advancement over traditional knee osteoarthritis treatments, such as physiotherapy, anti-inflammatory medications, and cortisone injections. Unlike standard options, which often offer diminishing returns and can actively damage the joint over time, orthobiologics work with your body’s own biology to address joint degeneration from the inside out.
This leads to a critical question: what is the difference between two of the most common biologic options, Platelet-Rich Plasma (PRP) and Adipose Therapy – such as Micro-Fragmented Adipose Tissue (MFAT) or Regenerative Matrix Therapy™?
Both are autologous (drawn from your own body) and injected into the joint. A key difference lies in what they’re made of:
- PRP is concentrated from blood and delivers a surge of growth factors to reduce inflammation, but its cellular content is limited.
- Adipose Tissue (such as in MFAT) has a considerably richer biological profile. It contains a complex mixture of mesenchymal stem cells, pericytes, endothelial cells, fibroblasts, and a dense network of growth factors. The goal is for the adipose tissue to directly treat the underlying causes of joint degeneration and potentially even reverse disease progression.
A 2022 prospective randomized controlled trial by Zaffagnini et al., published in the American Journal of Sports Medicine, confirmed that these treatments are not interchangeable, particularly for patients with moderate to severe disease.
Why Disease Severity Changes the Equation
To understand why MFAT and PRP perform differently in more advanced arthritis, it helps to understand what each treatment delivers to the joint — and what moderate-to-severe osteoarthritis actually requires.
Standard treatments like corticosteroids temporarily suppress inflammation but damage the joint environment and wear off. Hyaluronic acid lubricates surfaces but doesn’t address the underlying biology. PRP concentrates growth factors and signalling proteins from your blood and can meaningfully reduce inflammation.
Adipose tissue operates at a different biological level. Fat tissue contains a biologically rich mixture containing mesenchymal stem cells, fibroblasts, endothelial cells, extracellular matrix, and non-cell biological components, including a dense network of growth factors and exosomes. It directly treats the underlying causes of joint degeneration and works to potentially reverse disease progression.
This distinction becomes especially consequential as osteoarthritis advances. In moderate-to-severe disease, the joint environment is more deeply compromised — inflammation is more entrenched, structural changes are more significant, and the biological needs for recovery become more complex. Adipose therapy appears to meet that demand in a way that PRP often cannot.
This 2022 trial was a Level 1 randomized controlled trial — the gold standard of clinical research design — to directly compare these two biologics in the same patient population, with rigorous blinded evaluation, serial imaging, and validated outcome measures tracked across two full years.
Learn More About Regenerative Matrix Therapy™
Study Overview: MFAT vs. PRP — A Level 1 Head-to-Head Randomized Controlled Trial
Study Design: Prospective, single-blind randomized controlled trial (Level 1 evidence); treating clinicians and the evaluating musculoskeletal radiologist were blinded to treatment allocation throughout follow-up
Participants: Adults aged 18–75 with symptomatic knee OA (Kellgren-Lawrence grade 1–4); minimum three months of failed non-operative treatment
Sample Size: 118 patients randomized; 108 treated and included in analysis (53 MFAT, 55 PRP)
Severity Mix:
- MFAT group: KL Grade 1: 8 patients | KL Grade 2: 20 patients | KL Grade 3: 13 patients | KL Grade 4: 12 patients (mild OA: 28 patients; moderate/severe OA: 25 patients)
- PRP group: KL Grade 1: 9 patients | KL Grade 2: 16 patients | KL Grade 3: 18 patients | KL Grade 4: 12 patients (mild OA: 25 patients; moderate/severe OA: 30 patients)
Notable Baseline Observation: While the authors confirmed statistical homogeneity between groups (beyond a BMI difference), the MFAT group entered the trial with meaningfully lower scores on both primary outcome measures — IKDC subjective score (41.1 vs. 44.8) and KOOS pain subscore (58.4 vs. 63.5) — indicating a directionally worse functional starting point.
Intervention:
- MFAT group: Single intra-articular injection of 5 mL micro-fragmented adipose tissue, harvested from subcutaneous abdominal fat and processed via progressive mechanical fragmentation in a physiological solution
- PRP group: Single intra-articular injection of 5 mL PRP (outpatient clinic; double centrifugation protocol; target platelet concentration ~5× baseline whole blood values; activated with calcium gluconate)
Follow-Up: 1, 3, 6, 12, and 24 months
Primary Endpoints: IKDC subjective score and KOOS pain subscore at 6 months
Secondary Endpoints: Additional KOOS subscales (symptoms, ADL, sport/recreation, quality of life), EQ-VAS, EQ-5D, VAS pain, radiographic KL grading, MRI via Whole-Organ Magnetic Resonance Imaging Score (WORMS), MCID achievement rates, treatment failure (Kaplan-Meier), and subgroup analyses by OA severity (KL 1–2 vs. KL 3–4)
Key Findings: In Advanced Knee OA, MFAT Produced More Than Double the Response Rate of PRP
1. Meaningful Functional Improvement — From a Lower Starting Point
~38% improvement in IKDC subjective score (41.1 → 57.3; p < .0005)
Overall knee function improved substantially in the MFAT group at 6 months, spanning the full range of daily activities and recreational participation. Notably, this improvement was achieved from a baseline that was meaningfully lower than the PRP group’s starting point — yet both groups arrived at nearly identical endpoint scores. In practical terms, MFAT produced greater absolute gains from a more compromised starting position.
2. Clinically Significant Pain Relief, Sustained at Two Years
~29% improvement in KOOS pain score (58.4 → 75.8 at 6 months; p < .0005), with improvement maintained through 24 months (+10.0 points from baseline)
Pain reduction was clinically significant and durable. At two years, the MFAT group continued to demonstrate greater absolute improvement than the PRP group on both the IKDC (+12.7 vs. +8.7 points from baseline) and KOOS pain (+10.0 vs. +7.8 points from baseline), directionally reinforcing the durability of the treatment effect.
3. The Defining Finding: Advanced OA Responded Dramatically Better to MFAT
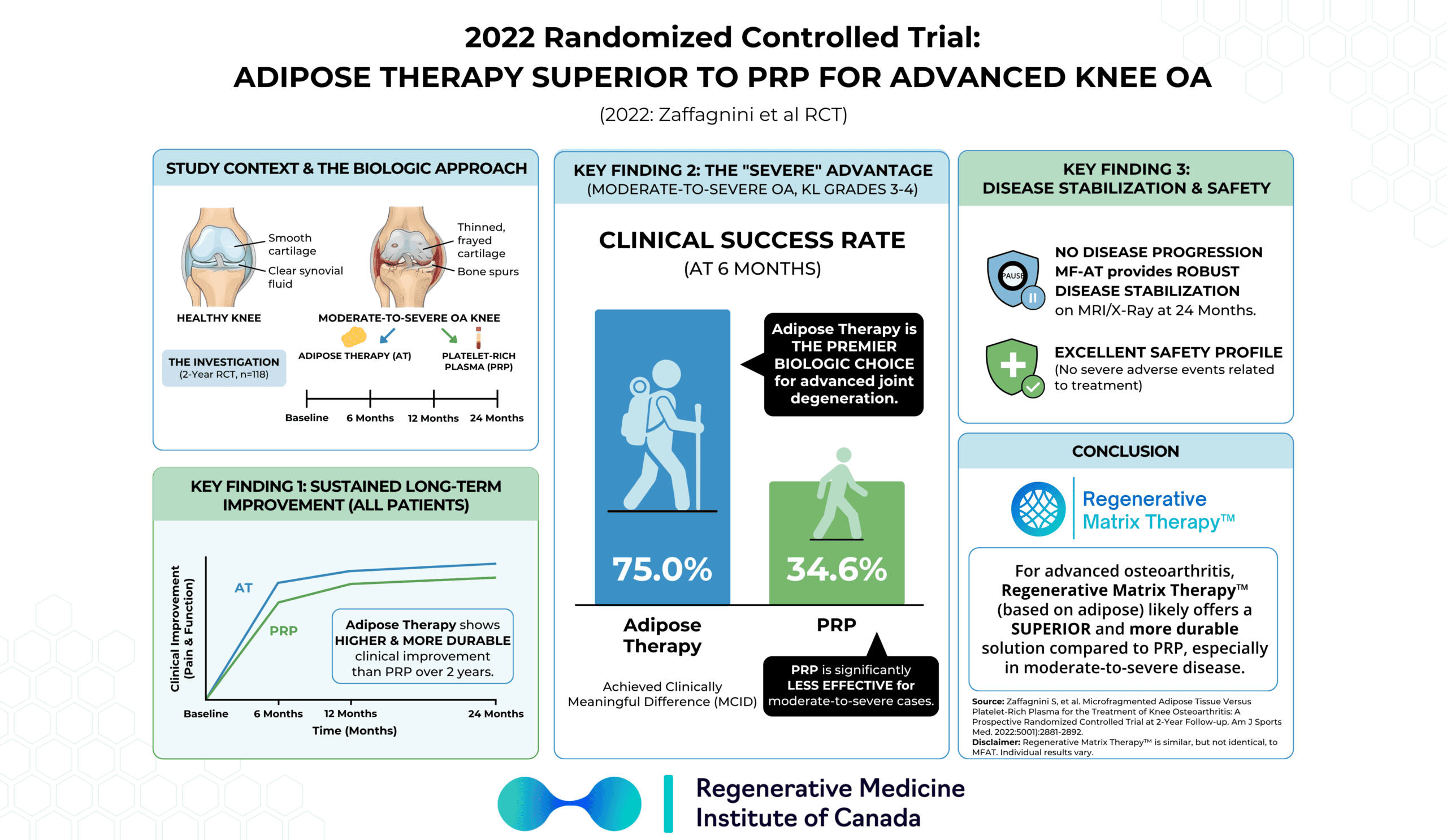
In patients with moderate or severe osteoarthritis (KL grade 3–4) — those with the most to gain from an effective biologic and most at risk of being told surgery is their only remaining option — MFAT produced more than double the clinically meaningful response rate of PRP at six months.
- MFAT: 75.0% of moderate/severe OA patients reached the minimal clinically important difference (MCID) on the IKDC score at 6 months
- PRP: 34.6% of moderate/severe OA patients reached the MCID at 6 months
- P = .005
In patients with moderate to severe knee osteoarthritis, the adipose-based biologic was more than twice as likely as PRP to produce a meaningful clinical response.
In patients with mild OA (KL 1–2), no significant difference was observed between treatments — suggesting PRP remains a reasonable option at earlier disease stages, while MFAT’s advantage becomes most pronounced as severity increases.
4. Overall MCID Achievement — A Consistent Advantage for MFAT
73.5% of all MFAT-treated patients achieved the MCID for the IKDC subjective score at 6 months, compared with 55.1% in the PRP group. For KOOS pain, 63.3% of MFAT patients reached the MCID at 6 months, compared with 44.9% in the PRP group.
5. Directionally Lower Treatment Failure Rate
The MFAT group showed a numerically lower treatment failure rate at 24 months — 15.1% vs. 25.5% in the PRP group — a difference that did not reach statistical significance in this sample but that directionally represents a meaningful reduction in treatment failures and warrants attention in future adequately powered studies.
6. No Disease Progression in Either Group
Serial radiographic evaluation (KL grading) and high-resolution MRI (WORMS scoring across seven structural features — including articular cartilage morphology, bone marrow edema, subchondral cysts, and synovitis) showed no deterioration in OA severity in either group at any follow-up point through 24 months. Neither treatment arrested structural progression, but critically, neither accelerated it — reinforcing the safety profile of both biologic approaches.
7. Well-Tolerated in Both Groups
Adverse events were predominantly mild and self-limiting in both groups — transient knee pain, joint swelling or effusion, and injection site discomfort — resolving within days and requiring no specific intervention or hospitalization. The overall adverse event rate was 18.9% in the MFAT group and 10.9% in the PRP group, with no statistically significant difference between groups. No treatment-related serious adverse events occurred in either group through 24 months.
What This Means for You
If you’ve been told you have moderate or severe knee osteoarthritis — the stages where physicians often start framing timelines to replacement — this trial offers something genuinely important: the highest level of clinical evidence showing that a fat-derived biologic can produce clinically meaningful improvement in your patient population, and that it outperforms the most established biologic comparator by a substantial margin.
For patients with moderate or severe arthritis, the numbers are striking. Three out of four patients who received the adipose-based biologic achieved a meaningful clinical response. Among those who received PRP, the figure was one in three. This demonstrated a real divergence in how these two treatments interact with a more compromised joint environment, and it points to a clear rationale for choosing MFAT over PRP as disease severity increases.
In moderate to severe knee osteoarthritis, the adipose-based biologic produced more than double the meaningful clinical response rate of PRP.
There is a secondary signal in this trial equally worth understanding. While the headline results showed both treatments arriving at statistically similar overall endpoints, the MFAT group began from a lower functional baseline on both primary outcome measures. Achieving equivalent outcomes from a worse starting position isn’t truly equivalent in any meaningful clinical sense — it reflects a pattern of superior absolute improvement that the group-level analysis couldn’t fully capture, and it is directionally consistent with what the subgroup analysis confirmed in moderate-to-severe patients specifically. This is an observational inference, not a proven conclusion from this trial alone, but it is a signal that aligns with the biological rationale for MFAT in more advanced disease.
It’s also worth acknowledging what the trial showed across the full patient population: both treatments were effective, safe, and associated with no disease progression at two years. For patients with earlier-stage arthritis, PRP remains a clinically reasonable option. The distinction becomes most consequential as severity increases — and that’s exactly the population who most needs clarity on which biologic to pursue.
RMIC’s proprietary Regenerative Matrix Therapy™ shares foundational similarities with, but is not identical to, the MFAT treatment studied in this trial. The results here are directionally supportive of the biologic approach we use — designed to engage your own biology to address the root causes of joint degeneration. RMIC’s proprietary Regenerative Matrix Therapy™ protocol has been reviewed by Health Canada with no objection.
Start Your Virtual Consultation
Research Highlights (For Clinicians)
Study Citation: Zaffagnini S, Andriolo L, Boffa A, et al. Microfragmented Adipose Tissue Versus Platelet-Rich Plasma for the Treatment of Knee Osteoarthritis: A Prospective Randomized Controlled Trial at 2-Year Follow-up. Am J Sports Med. 2022;50(11):2881–2892. DOI: 10.1177/03635465221115821
Study Design: Single-blind prospective RCT (Level 1 evidence); computer-generated 1:1 randomization. Assessors (clinicians conducting follow-up evaluations) and an independent musculoskeletal radiologist blinded to treatment allocation. MFAT performed as a single surgical step in the operating room; PRP administered in the outpatient clinic — patient blinding not feasible given procedural differences. External independent agency (PHARM srl, Lodi, Italy) verified data integrity and correctness.
Population: n = 108 treated and analyzed (53 MFAT, 55 PRP); mean age 54.5 ± 12.1 (MFAT) and 54.1 ± 10.6 (PRP). KL grade 1–4 throughout; mild OA (KL 1–2): MFAT 28/53 (52.8%), PRP 25/55 (45.5%); moderate/severe OA (KL 3–4): MFAT 25/53 (47.2%), PRP 30/55 (54.5%). Baseline IKDC: 41.1 ± 16.3 (MFAT) vs. 44.8 ± 17.3 (PRP); KOOS pain: 58.4 ± 15.9 (MFAT) vs. 63.5 ± 17.8 (PRP). Only statistically significant baseline difference: BMI (MFAT 25.9 ± 4.3 vs. PRP 28.0 ± 5.5; P = .031), with both groups classified as overweight by CDC criteria.
Intervention:
- MFAT (Lipogems®): Single intra-articular injection of 5 mL MFAT processed via the Lipogems® system (Lipogems International Spa, Milan, Italy). Subcutaneous abdominal fat harvested via 13-gauge blunt cannula connected to a 20-mL Vaclock syringe; local anaesthesia with adrenaline and lidocaine in 500 mL saline. Progressive mechanical fragmentation in complete physiological solution immersion; elimination of oily substances, cell debris, and blood residue. No enzymatic treatment. Injected via 18-gauge needle, lateral parapatellar approach, knee in extension.
- PRP: 150 mL peripheral venous blood; double centrifugation (1480 rpm × 6 min; 3400 rpm × 15 min); platelet-poor plasma manually removed; target platelet concentration 1000 × 10³/mL ± 20% (~5× baseline whole blood); mean leukocyte concentration ~1.5× whole blood. Stored frozen at −30°C; thawed at 37°C for 30 min; activated with 1 mL calcium gluconate. Single injection via 22-gauge needle, lateral parapatellar approach.
Primary Outcome Effects — IKDC Subjective Score at 6 Months:
- MFAT: 41.1 ± 16.3 → 57.3 ± 18.8 (+15.8 points; p < .0005)
- PRP: 44.8 ± 17.3 → 58.4 ± 18.1 (+13.6 points; p < .0005)
- Intergroup comparison: NS
Primary Outcome Effects — KOOS Pain Subscore at 6 Months:
- MFAT: 58.4 ± 15.9 → 75.8 ± 17.4 (+16.8 points; p < .0005)
- PRP: 63.5 ± 17.8 → 75.5 ± 16.1 (+12.3 points; p < .0005)
- Intergroup comparison: NS
Longitudinal IKDC Improvement (mean change from baseline, all p < .05 vs. baseline within groups):
- MFAT: +12.5 ± 13.9 (3M) | +15.8 ± 16.9 (6M) | +12.8 ± 19.2 (12M) | +12.7 ± 17.8 (24M)
- PRP: +11.1 ± 15.4 (3M) | +13.6 ± 15.4 (6M) | +13.2 ± 17.6 (12M) | +8.7 ± 18.5 (24M)
- Intergroup: NS at all timepoints
Longitudinal KOOS Pain Improvement (mean change from baseline):
- MFAT: +9.5 ± 18.7 (3M) | +16.8 ± 16.4 (6M) | +11.4 ± 16.4 (12M) | +10.0 ± 17.6 (24M)
- PRP: +8.6 ± 15.7 (3M) | +12.3 ± 17.9 (6M) | +12.6 ± 18.7 (12M) | +7.8 ± 17.7 (24M)
- Intergroup: NS at all timepoints
MCID Rates — IKDC:
- MFAT: 73.5% at 6M; 60.4% at 12M
- PRP: 55.1% at 6M; 56.0% at 12M
MCID Rates — KOOS Pain:
- MFAT: 63.3% at 6M; 56.3% at 12M
- PRP: 44.9% at 6M; 50.0% at 12M
Critical Subgroup — Moderate/Severe OA (KL 3–4):
- IKDC improvement at 6M: MFAT +15.7 ± 19.0 vs. PRP +8.6 ± 14.2 (P = .041); not confirmed at 12M (+10.0 ± 21.7 vs. +10.1 ± 18.6; NS) or 24M (+9.3 ± 17.4 vs. +5.6 ± 19.1; NS)
- MCID for IKDC at 6M: MFAT 75.0% vs. PRP 34.6% (P = .005); not replicated at 12M (52.2% vs. 46.4%; NS)
- KOOS pain MCID at 6M: MFAT 58.3% vs. PRP 42.3% (NS); 12M: 43.5% vs. 46.4% (NS)
Mild OA Subgroup (KL 1–2): No statistically significant intergroup differences at any timepoint. Within the PRP group, mild OA patients showed significantly greater IKDC improvement vs. moderate/severe OA patients (19.2 ± 15.0 vs. 8.6 ± 14.2; P = .014) and higher MCID rate (78.3% vs. 34.6%; P = .002).
Treatment Failure (Kaplan-Meier, 24M):
- MFAT: 15.1% (8/53) — 3 repeat injections, 3 TKA, 2 unicompartmental knee replacement
- PRP: 25.5% (14/55) — 9 repeat injections, 5 TKA
- Intergroup comparison: NS
Imaging Outcomes — WORMS (7 structural features: articular cartilage morphology, bone marrow edema, subchondral cysts, articular profile, marginal osteophytes, meniscal integrity, synovitis): No significant change in any feature in either group at 6, 12, or 24 months; no intergroup difference. Radiographic KL grading likewise showed no deterioration in OA severity at any follow-up in either group.
Outcome Predictors (MFAT group): Younger age correlated with greater KOOS pain improvement at 24M (rho = −0.317; P = .026). Better baseline WORMS values (less bone marrow edema, less synovitis) correlated with better IKDC, VAS, KOOS pain, symptoms, and ADL at 12M (all P < .05). Superior baseline articular cartilage morphology (WORMS-1) correlated with better KOOS pain and ADL at 12M (P = .008 and P = .027).
Outcome Predictors (PRP group): Longer symptom duration correlated with worse KOOS pain (P = .035), VAS (P = .023), and EQ-VAS (P = .040) at 12M. Younger age correlated with better IKDC (P = .048), KOOS pain (P = .047), KOOS ADL (P = .033), and EQ-5D (P = .039) at 12M. Female sex associated with greater IKDC, KOOS ADL, and EQ-5D improvement at 24M (P = .023, .005, .005 respectively). Better baseline articular cartilage morphology (WORMS-1) correlated with better IKDC and KOOS pain at 6 and 12M (all P < .05).
Safety:
- MFAT: 18.9% adverse event rate; 10 mild AEs (knee pain, joint swelling/effusion, injection site pain — all self-limiting within days, none requiring intervention); 1 severe AE (leg edema secondary to patient non-compliance with compression band — hospitalization for 1 day, resolved with oral analgesics); 1 unrelated death at 24M (pulmonary embolism post-prostatectomy, confirmed unrelated to treatment)
- PRP: 10.9% adverse event rate; 6 mild AEs (knee pain, joint swelling/effusion, injection site pain — all self-limiting); no severe AEs
- Intergroup AE rate: NS
Limitations:
- Single-blind design only (patient blinding not feasible given OR-based MFAT vs. outpatient PRP; clinician and radiologist blinding maintained)
- Higher dropout rate than pre-specified in power calculation; some follow-up delays attributable to COVID-19 pandemic (affected both groups comparably)
- No placebo/sham control arm — PRP selected as active comparator based on its documented superiority over saline, corticosteroids, and hyaluronic acid
- OA severity subgroup analyses were exploratory in design
- Single-injection protocol; no repeat injection data available — the role of re-treatment in sustaining or extending the response remains unknown
Learn More About Regenerative Matrix TherapySee More Conditions We Treat
Disclaimer
This content is intended for educational purposes only and does not constitute medical advice or a substitute for consultation with a qualified healthcare provider. Individual results vary based on disease severity, anatomy, and adherence to post-care protocols. Regenerative Matrix Therapy™ shares foundational similarities with, but is not identical to, the treatment studied in this trial.
Why Choose Regenerative Matrix Therapy™ With RMIC?
RMIC’s Regenerative Matrix Therapy™ is delivered through a standardized, physician-led protocol designed to harness your own biology to address joint degeneration at its source. RMIC’s proprietary Regenerative Matrix Therapy™ protocol has been reviewed by Health Canada with no objection. If you’re navigating the treatment gap between failed conservative care and surgery you’re not ready for, we invite you to explore whether you’re a candidate.