2021 Large Study: Adipose Therapy Works Even in Severe Knee OA — With Women Responding Best
One of the Largest MFAT Studies — and What It Reveals About Who Responds Best
For years, the central question in regenerative orthopedics has been a relatively simple one: does it work? Study after study on adipose therapy for knee osteoarthritis has answered with consistent affirmations — meaningful reductions in pain, measurable improvements in function, and a genuine return to activity for patients who had exhausted conventional options.
A large 2021 study published in Stem Cells International by Borg, Heidari, and colleagues adds important nuance to that record. Analyzing 418 patients who received intra-articular MFAT injections for knee osteoarthritis — one of the largest observational cohorts in the adipose therapy literature — the researchers applied a rigorously bias-mitigated statistical framework to examine whether men and women respond differently to treatment.
For both groups, the treatment worked. Men showed a 60% pain response rate and 65% functional response rate at two years — meaningful outcomes in a cohort where the majority of patients presented with the most severe grade of knee OA. But the results for women were in a different category entirely.
Women responded to treatment at a 90% rate for pain improvement, compared to 60% for men. They demonstrated nearly three times the pain reduction and nearly three times the functional gain at two years. And they achieved this despite starting in worse condition — reporting higher pain and lower function at baseline than their male counterparts, then surpassing men on both measures by the two-year mark.
This research matters beyond any single comparison. As adipose therapy matures as a field, studies like this one shift the conversation from “does it work?” toward “for whom, how much, and why?” — the essential questions of precision medicine. The data doesn’t just confirm a treatment. It begins to draw a more detailed map of who stands to benefit most.
The Biology Behind the Benefit — and Why It Differs Between Patients
To understand why these differences exist, it helps to first understand what adipose therapy actually does — and why it operates so differently from the conventional approaches your knee has likely already seen.
Your adipose tissue contains a rich concentration of biological components – including mesenchymal stem cells, fibroblasts, endothelial cells, extracellular matrix, and non-cell biological components – that, when harvested, processed, and injected directly into a damaged joint, address the underlying causes of osteoarthritic pain rather than simply masking them. Where a cortisone injection suppresses inflammation temporarily while also damaging the joint environment over time, and where hyaluronic acid acts more like motor oil than medicine — lubricating without repairing — adipose therapy draws on your own biology to target the smoldering chemical breakdown driving your symptoms. The goal isn’t to cover the problem. It’s to engage the body’s own tissue to fix it.
But biology isn’t uniform. Men and women experience OA differently, and there is growing evidence across medicine that men and women respond differently to both surgical and non-surgical treatments. Hormonal and metabolic differences between the sexes are understood to influence how the joint environment responds to biological stimulation, though the specific mechanisms underlying the gender difference in adipose tissue response require further investigation.
This is precisely what makes studies like Borg et al. so valuable. Understanding that patients don’t all respond identically — and beginning to map who benefits most, and why — is how a promising therapy becomes a precise one.
Learn More About Regenerative Matrix Therapy™
Study Overview: Gender-Specific Response to MFAT at Two Years
Study Design: Observational, intention-to-treat cohort. Single arm, no control group. Private practice clinical setting (London, UK). Gender-bias mitigation applied via random undersampling of the larger male cohort; Bayesian statistical analysis (BEST package) used to estimate credible differences in means between groups. Missing data handled via multiple imputation using the Amelia II package (17% MCAR rate). All analysis performed in open-access R software for reproducibility.
Participants: Adults presenting with knee pain and radiographically confirmed osteoarthritis. Mean age: 66±12 years (women), 65±12 years (men). Inclusion required ≤10° varus/valgus deformity and confirmed OA on X-ray or MRI. Exclusion criteria included recent knee injury within 3 months, infectious joint disease, malignancy, pregnancy, anticoagulation, and intra-articular steroid injection within 3 months.
Sample Size: Full dataset: 418 knees. Gender-bias-mitigated analytical cohort: 192 women and 194 men (n=386). 17% missing data rate at later follow-up timepoints.
Severity Mix: Median KL grade 3 in both groups. Women (post-mitigation): KL I=6, KL II=40, KL III=42, KL IV=104. Men (post-mitigation): KL I=7, KL II=33, KL III=50, KL IV=104. The majority of patients in both groups presented at KL grade IV, the most severe classification — a population that would typically be considered candidates for knee arthroplasty.
Intervention: Adipose tissue harvested under sedation via mini-liposuction and processed into MFAT. Injected under ultrasound guidance into the affected knee joint. Performed in an operating theatre as a day case. Physiotherapy protocol provided post-procedure.
Follow-Up: 3 months, 6 months, 1 year, and 2 years.
Endpoints: Primary — VAS pain score (0–100; lower = better) and Oxford Knee Score (OKS; 0–48; higher = better). Responder classification applied: VAS superresponder threshold = ≥20-point improvement; OKS superresponder threshold = ≥7-point improvement (both aligned with published MCID thresholds).
Key Findings: Meaningful Improvement for All — and a Striking Advantage for Women
1. Both Men and Women Experienced Clinically Meaningful Improvement
At two years, both groups showed genuine gains. Men’s average pain scores dropped from 41.0 to 31.0 on the VAS, and functional scores improved from 32.0 to 38.0 on the Oxford Knee Score — with 60% responding for pain and 65% for function, and 40% and 38% reaching superresponder thresholds, respectively. For a cohort where the majority of patients presented at the most severe grade of knee OA, these are outcomes that translate into real changes in daily life: less reliance on pain medication, more confidence on stairs, a broader range of tolerable activity.
Women improved across the same measures — and then some. Their results were in a different category entirely, and that gap is the central finding of this study.
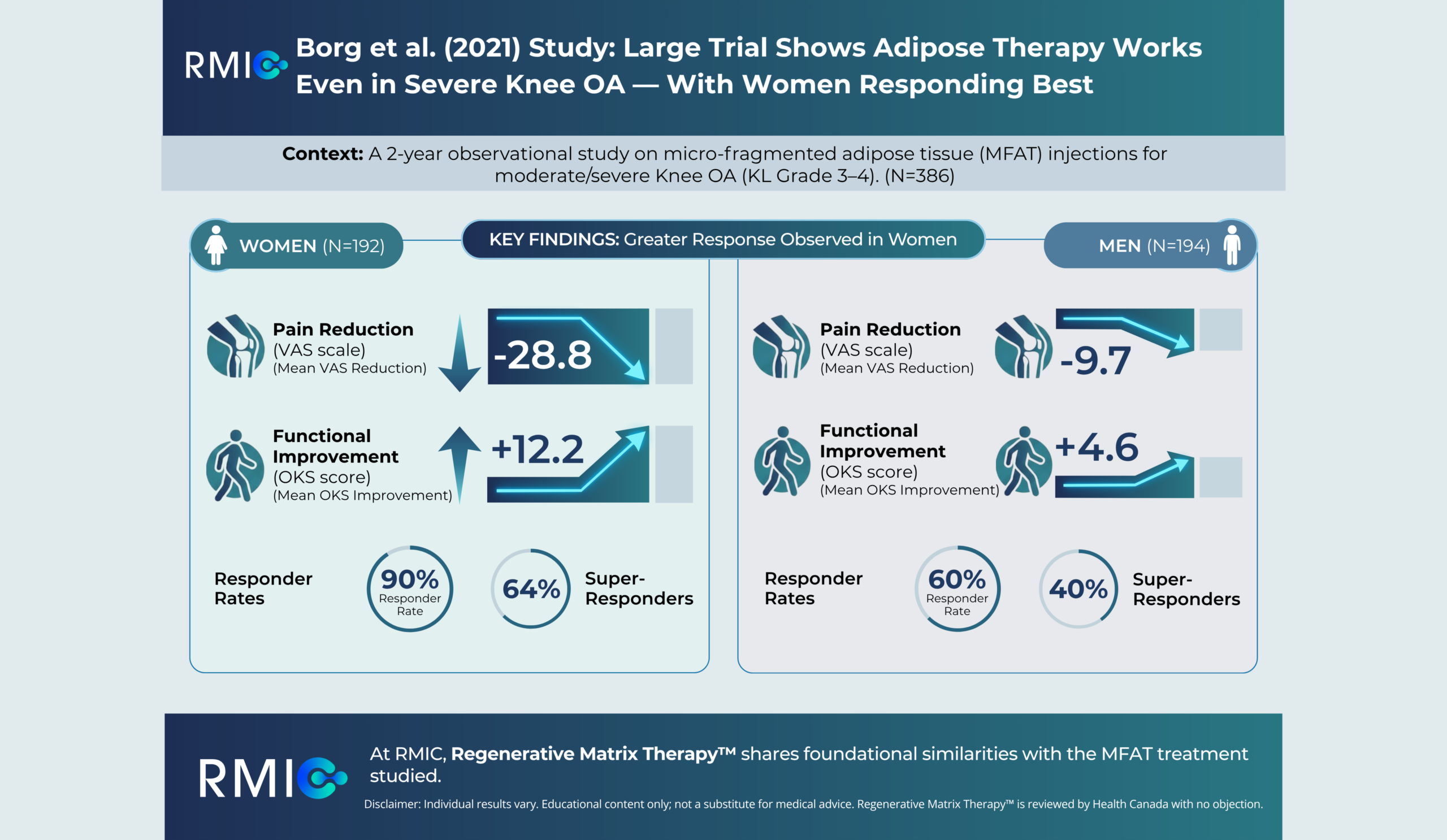
2. Women Reduced Pain by Nearly Three Times More Than Men
Women: mean VAS dropped from 49.0 to 28.0 at two years (Bayesian credible reduction: −28.8 points, 95% credible interval: −34.4 to −23.6). Men: mean VAS dropped from 41.0 to 31.0 (Bayesian credible reduction: −9.7 points, 95% credible interval: −16.0 to −3.0).
Women entered treatment carrying significantly more pain than men — and by two years had lower pain scores than men had reached. That reversal is the clearest signal in the data. For many women in this cohort, a reduction of that magnitude translates to sleeping through the night, navigating stairs without bracing, and reclaiming activities that had been quietly set aside.
3. Women’s Functional Improvement Was Nearly Three Times Greater
Women: OKS improved from 27.0 to 36.0 (Bayesian credible improvement: +12.2 points, 95% credible interval: +10.3 to +14.1). Men: OKS improved from 32.0 to 38.0 (Bayesian credible improvement: +4.6 points, 95% credible interval: +2.5 to +6.8).
The Oxford Knee Score spans 12 domains of daily function — walking, stair-climbing, pain during rest and activity. A 12-point gain for women far exceeds the MCID superresponder threshold of 7 points and represents one of the more clinically significant functional improvements documented in the MFAT literature.
4. 9 in 10 Women Responded — Most at a Superresponder Level
90% of women demonstrated meaningful improvement in pain, with 64% classified as superresponders — achieving the ≥20-point VAS reduction threshold for clinically significant change. For function, 87% of women responded on the OKS, with 70% reaching superresponder status (≥7-point improvement). These response rates, alongside the magnitude of improvement, make the female cohort’s results among the most consistent in observational MFAT research to date.
5. Women Overcame a Worse Starting Point
At baseline, women reported more pain (VAS 49 vs. 41) and worse knee function (OKS 27 vs. 32) than men. Despite arriving at treatment in greater distress, they surpassed men on both pain and functional outcomes at two years — not simply closing the gap, but exceeding male outcomes across every measure.
6. Safety Profile Was Acceptable Across Both Groups
Adverse events were mild and infrequent. The most common were transient joint pain (approximately 9% in both groups) and discomfort at the fat harvest site (approximately 3–4%). One serious adverse event was recorded — a female patient who required knee washout at another institution due to persistent pain and inflammation. No systemic complications or treatment-related infections were reported.
What This Means for You
Even among patients with the most advanced knee OA — including bone-on-bone disease — both men and women in this study experienced meaningful, lasting improvement, with women achieving outcomes that stand among the strongest documented in the MFAT literature.
The majority of patients in this 418-person cohort presented at Kellgren-Lawrence grade IV — the most severe classification of knee osteoarthritis, where cartilage loss is effectively complete and patients are typically steered toward joint replacement. Yet both men and women responded. Men showed a 60% pain response and 65% functional response rate at two years. Women achieved a 90% pain response and 87% functional response. These are not marginal results in a mild-to-moderate population. They are clinically meaningful outcomes in a cohort of patients many would have considered beyond the reach of non-surgical intervention.
For women, the picture is even more striking. 9 in 10 women experienced meaningful pain relief, and 7 in 10 reached super-responder status for function — the threshold for changes significant enough to materially alter daily life. Women entered treatment in more pain and with worse joint function than their male counterparts and, two years later, had surpassed men on both measures. The data suggests that women may carry a biological profile — hormonal and metabolic — that amplifies the response to adipose-based therapy in ways that are only beginning to be understood and studied.
For men, the story is one of genuine, clinically important benefit in a population with severe disease. For women, it is that and considerably more.
Both findings point in the same direction: adipose therapy is not a treatment reserved for mild OA or for patients willing to accept modest gains. This study’s data suggests it can produce significant outcomes even at the most advanced end of the disease spectrum — and that for women in particular, the benefit can be remarkable.
RMIC’s proprietary Regenerative Matrix Therapy™ shares foundational similarities with the MFAT-based treatment studied by Borg et al. — but is not identical to it. RMIC’s protocol is designed to engage your own biology and has been reviewed by Health Canada with no objection. It is delivered by a physician-led team using a standardized, evidence-informed approach.
Start Your Virtual Consultation
Research Highlights (For Clinicians)
Study Citation: Borg TM, Heidari N, Noorani A, Slevin M, Cullen A, Olgiati S, Zerbi A, Danovi A, Wilson A. “Gender-Specific Response in Pain and Function to Biologic Treatment of Knee Osteoarthritis: A Gender-Bias-Mitigated, Observational, Intention-to-Treat Study at Two Years.” Stem Cells International. 2021;2021:6648437. DOI: 10.1155/2021/6648437
Study Design: Observational, intention-to-treat cohort. Single arm, no control group. Private practice (The Regenerative Clinic, London, UK). Gender-bias mitigation performed via random undersampling to balance male and female cohort sizes (Amelia II multiple imputation for 17% MCAR missing data). Bayesian analysis (BEST package, Kruschke methodology) used to estimate credible differences in means between genders, with minimally informative priors. All analysis conducted in open-access R software (v4.0.3+) for reproducibility and replicability.
Population: Full dataset: n=418 knees. Post-gender-bias-mitigation analytical cohort: n=386 (192 female, 194 male). Mean age: 66±12 (F), 65±12 (M). Median KL grade 3 in both groups. KL distribution post-mitigation — Female: KL I=6, KL II=40, KL III=42, KL IV=104. Male: KL I=7, KL II=33, KL III=50, KL IV=104. Both cohorts heavily weighted toward KL grade IV. Mean BMI: 28±5 (F), 27±4 (M). Median ASA grade 2 in both groups.
Intervention: Adipose tissue harvested under sedation via mini-liposuction and processed using the Lipogems® system into MFAT. Ultrasound-guided intra-articular injection into the affected knee. Performed in OR as a day case. Standardized physiotherapy protocol provided post-procedure.
Effect Sizes — VAS (0–100, lower = better):
- Women: preop 49.0 → 2-year 28.0; Bayesian credible reduction: −28.8 (95% CI: −34.4 to −23.6)
- Men: preop 41.0 → 2-year 31.0; Bayesian credible reduction: −9.7 (95% CI: −16.0 to −3.0)
Effect Sizes — OKS (0–48, higher = better):
- Women: preop 27.0 → 2-year 36.0; Bayesian credible improvement: +12.2 (95% CI: +10.3 to +14.1)
- Men: preop 32.0 → 2-year 38.0; Bayesian credible improvement: +4.6 (95% CI: +2.5 to +6.8)
Responder / Superresponder Rates (VAS superresponder: ≥20-point improvement; OKS superresponder: ≥7-point improvement — both at published MCID threshold):
- Female VAS: 90% responder (164/192); 64% superresponder (123/192)
- Male VAS: 60% responder (117/194); 40% superresponder (78/194)
- Female OKS: 87% responder (167/192); 70% superresponder (134/192)
- Male OKS: 65% responder (126/194); 38% superresponder (74/194)
Safety (reported from full pre-mitigation dataset):
- Joint swelling or pain: 9% female (19/192 pre-mitigation), 9% male
- Pain at fat harvest site: 3% female, 4% male
- Harvest site bleeding: 1% in both groups
- Serious AE: one female patient required knee washout at an external institution due to persistent pain and inflammation (details not available to authors); no fatalities or systemic complications reported
Limitations:
- Single-arm observational design; no control or comparator group
- 17% missing data rate at later timepoints, mitigated via multiple imputation (Amelia II) — acknowledged as a residual potential source of bias
- Unquantified confounders including ethnicity, age strata, BMI, and KL grade not incorporated into gender-stratified analysis; authors identify these as subjects for future work
- Genomic, hormonal, and serum marker profiles (e.g., estrogen, leptin, parathyroid hormone, growth hormone) not measured or included — the proposed mechanistic explanations for the gender differential are therefore inferential
- Single private-practice clinical setting; self-selected patient population limits generalizability
Learn More About Regenerative Matrix Therapy™See More Conditions We Treat
Disclaimer
This content is intended for educational purposes only and does not constitute medical advice or a substitute for consultation with a qualified healthcare provider. Individual results vary based on disease severity, anatomy, and adherence to post-care protocols. Regenerative Matrix Therapy™ shares foundational similarities with, but is not identical to, the treatment studied in this trial.
Why Choose Regenerative Matrix Therapy™ With RMIC?
RMIC’s Regenerative Matrix Therapy™ is delivered through a standardized, physician-led protocol built on a rigorous and growing body of adipose therapy evidence. Our proprietary protocol has been reviewed by Health Canada with no objection. If you’re navigating the treatment gap between failed conservative care and surgery you’re not ready for, we invite you to explore whether you’re a candidate.