2023 Study: Adipose Therapy Outperforms Hyaluronic Acid for Knee OA
Conventional Therapy: Hyaluronic Acid
It is a familiar and frustrating cycle for anyone trying to maintain an active lifestyle with knee osteoarthritis. You feel the familiar ache, you visit the clinic, and you are offered a lubricating gel injection, commonly known as Hyaluronic Acid (HA) or viscosupplementation. For a few months, you might feel a reprieve. You may initially enjoy activities like golfing or skiing with relief, but this relief inevitably fades. Stiffness and ache return, putting you back in a clinical holding pattern–trying to manage the decline of your joint and hoping to delay major joint replacement surgery for as long as possible.
For years, this cycle of temporary lubrication has been the standard of care. But modern orthobiologic research is fundamentally shifting how we approach joint preservation.
A landmark 2023 multicenter randomized controlled trial published in the World Journal of Stem Cells took a hard look at this standard approach. The researchers asked a pivotal question: What happens when we stop simply lubricating a degrading joint, and instead introduce a patient’s own biological tissue to the environment?
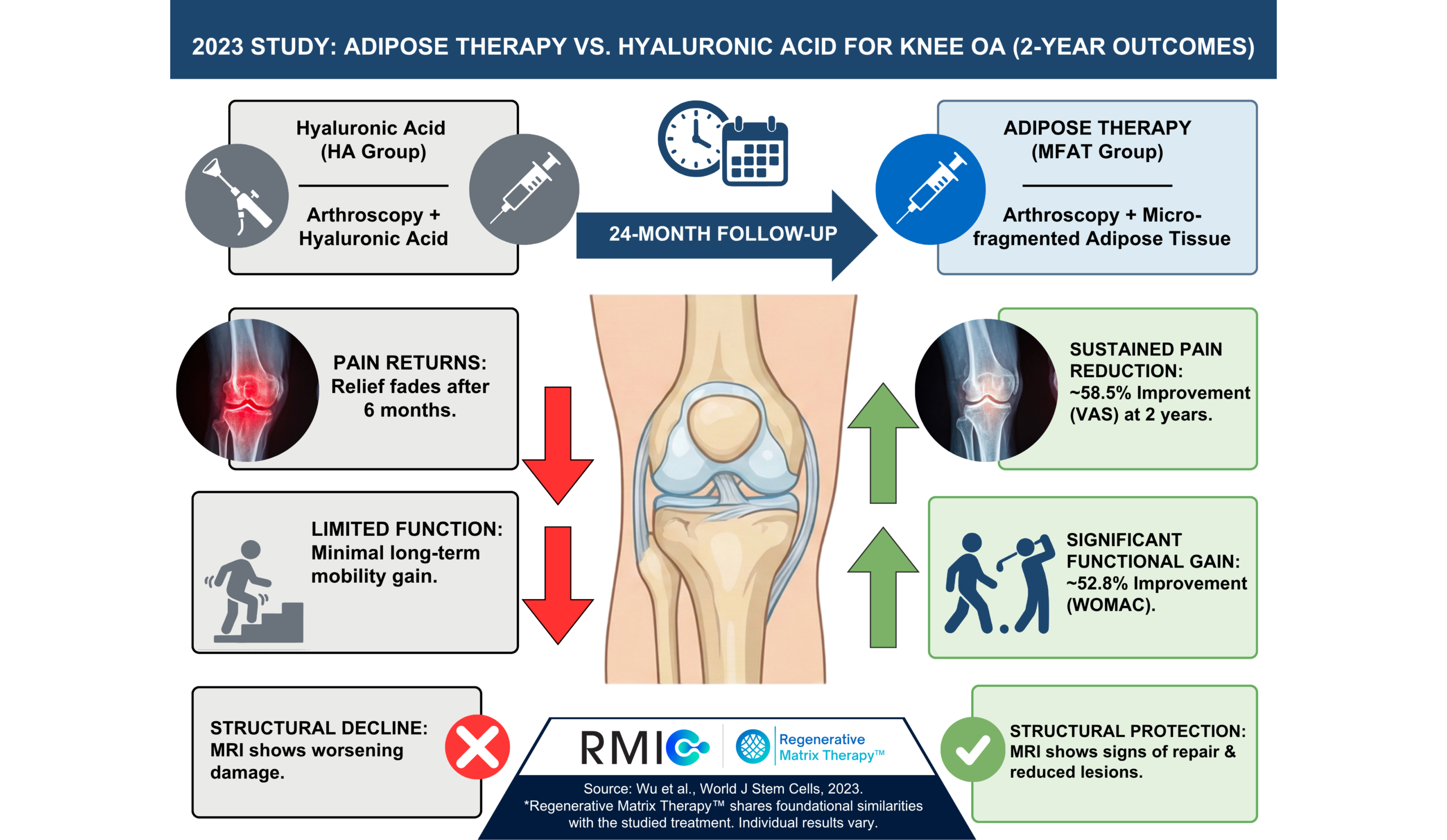
By directly comparing Hyaluronic Acid (HA) against Micro-Fragmented Adipose Tissue (MFAT)—both administered following a standard joint clean-out procedure (known as arthroscopy)—this study provides compelling, long-term evidence that harnessing your own biology offers a superior pathway to lasting relief.
The Anatomy of the Problem: The Protection Gap
To understand why gel injections eventually fail, we must look at the biological reality of an arthritic knee.
When osteoarthritis takes hold, the natural protection of the bones within the joint degrades. The joint becomes inflamed—a smoldering chemical fire that actively breaks down cartilage.
Traditional care attempts to address this mechanically. A surgeon might use arthroscopy to physically clean out the loose debris in the joint, followed by an injection of Hyaluronic Acid. HA acts like motor oil; it temporarily lubricates the mechanical parts. However, it is an inert substance. It does not replace the lost biological matrix, nor does it change the underlying inflammatory environment. The joint’s own inflammatory enzymes make HA less effective, causing the pain and friction to return.
This creates a significant protection gap. Adipose therapy aims to bridge this gap not by adding artificial oil, but by introducing a biological matrix derived from your own body, designed to support the joint in a way that synthetic gels simply cannot.
Learn More About Regenerative Matrix Therapy™
Study Overview: MFAT Plus Arthroscopy vs Arthroscopy Plus Hyaluronic Acid
The 2023 trial is highly significant due to its rigorous design, vast scope, and extended follow-up period. Wu et al. conducted a prospective, randomized, active-control, single-blind multicenter clinical trial across 10 hospitals in Zhejiang, China.
Study Design
Design and setting: Prospective, randomized, active-control, single-blind (observer-blinded) trial across 10 hospitals.
Participants: Adults aged 30–80 years with knee osteoarthritis symptoms for more than 6 months and mechanical or meniscal-type symptoms.
Sample size: 302 randomized patients across 10 different hospitals, with 151 per group; analysis tables reported 146 knees per group for outcomes reporting.
Follow-up: Outcomes were tracked at 6, 12, and 24 months.
Completion: 87.3% completed 24-month follow-up, with outcomes analyzed using intention-to-treat and last observation carried forward for missing data.
Severity Mix: This was not an end-stage “bone-on-bone” population. This study looked at moderate OA – only Kellgren–Lawrence grade 2–3 knees were included.
- MFAT group: 54.8% KL grade 2 (80/146); 45.2% KL grade 3 (66/146)
- Control group: 63.7% KL grade 2 (93/146); 36.3% KL grade 3 (53/146)
Notably, the severity mix between the two groups was not identical. The MFAT group contained a higher proportion of patients with advanced, Grade 3 osteoarthritis compared to the HA group. They started from a structurally worse baseline, making the final outcomes even more remarkable.
Intervention / Technique: All patients in the study underwent knee arthroscopy as a baseline intervention.
- MFAT arm: Abdominal fat harvested (liposuction), processed with Lipogems®, then injected into the knee during the same operative encounter (final product transferred to 10 mL syringes; exact injected volume not explicitly stated).
- Control arm: Three HA injections, 5 mL each, given once monthly after arthroscopy.
Endpoints:
- Primary endpoint: Change in WOMAC total score from baseline to 24 months.
- Secondary endpoints:
-
- WOMAC subscales
- VAS pain
- Lequesne index
- MRI WORMS (Whole-Organ Magnetic Resonance Imaging Score)
Key Findings: Biology Outperformed HA
The researchers tracked pain, joint stiffness, physical function, and even structural changes visible on MRI.The key message from this trial is that across the board, the biologic adipose treatment demonstrated clear superiority over the standard HA gel injections, even despite the MFAT group’s more severe starting condition.
1. Pain Relief Was Stronger and More Durable
While both groups experienced early improvement, the longevity of that relief diverged drastically. The adipose group experienced deep, sustained relief that held strong at the two-year mark, while the control group’s scores began to creep back up after the 6-month mark.
- Overall Pain Reduction: Pain improved by ~58.5% (VAS 5.3 → 2.2; p < 0.001) in the adipose group at 24 months. This was significantly better than the HA group (p = 0.006). On the WOMAC pain subscore, pain improved by 59% with MFAT (9.8 → 4.0) versus 38% with HA (9.5 → 5.9); p < 0.001.
The difference was short-lived improvement with HA versus relief that remained meaningful two years later with adipose/MFAT.
2. Overall Symptoms Improved More With MFAT
The study’s primary endpoint, the WOMAC total score, showed a highly significant improvement favoring the MFAT group over the HA group across all follow-up points.
- At 24 months, the MFAT group demonstrated a ~53% improvement in the WOMAC total score (48.3 → 22.8, p < 0.001). In comparison, the control group’s score improved by ~32% (from 46.5 to 31.7).
This is a critical finding, as the WOMAC score comprehensively captures the broader arthritis experience, including pain, stiffness, and functional limitation.
3. Dramatic Functional Gains Also Favoured MFAT over HA
Maintaining your everyday function and returning to the activities you love is the true measure of success. Using the various subscale scores, the study tracked the lifestyle improvements of the two patient groups.
- Restoring Mobility: On the WOMAC function subscale, patients in the MFAT group experienced a ~51% improvement (35.3 → 17.2) vs a ~30% improvement (33.8 → 23.6) in the HA group; p < 0.001.
- Reducing Morning Resistance: The WOMAC stiffness subscore improved by ~50% in the MFAT group (3.2 → 1.6) vs ~33% in the HA group (3.3 → 2.2); p < 0.001 at 24 months.
- Higher Quality of Life: The Lequesne index, a measure of disability and quality of life, improved by ~33% (10.7 → 7.2) in the MFAT group, compared with ~20% (10.3 → 8.2) in the HA group (p = 0.004 at 24 months).
Across all these subscores, the adipose group statistically outperformed the HA group at every major follow-up interval. Together, these findings show a consistent pattern: across pain, stiffness, disability, and daily function, MFAT outperformed hyaluronic acid when both were added to arthroscopy.
That kind of change may translate into easier stairs, longer standing tolerance, and more confidence loading the knee in everyday life. It does not mean the knee is “fixed,” but it does suggest that function can improve in ways that matter outside the clinic.
4. MRI Findings Showed Structural Protection
Perhaps the most interesting finding from this study on the power of adipose tissue came from the MRI data, evaluated using the WORMS (Whole-Organ Magnetic Resonance Imaging Score) system, which looks at the health of the cartilage and bone marrow.
Despite the fact that the adipose group started with a higher percentage of severe (Grade 3) arthritis, the following structural outcomes were observed:
- Decline in the HA Group: The HA control group saw their structural scores worsen over the two years (WORMS score increased: 60.8 → 62.1), which is the expected natural progression of osteoarthritis.
- Structural Improvement with Adipose: The adipose/MFAT group saw their structural scores actually improve (WORMS score decreased: 58.9 → 55.0; p = 0.020).
The MFAT group also demonstrated reduced femoral and tibial bone marrow lesions and improved osteochondral defects, and the authors described a higher proportion of MFAT patients with MRI features such as reduced bone marrow lesions and improved meniscus or osteochondral defect – signals of a healthier overall joint environment, a feat that standard HA lubrication cannot achieve.
5. Reassuring Safety Profile
There were no serious adverse events in either group.
Non-serious adverse events were comparable between groups. In the MFAT group, 5.4% (8 knees) experienced effusion, pain, or swelling lasting more than 5 days. In the control group, the rate was 6.2% (9 knees). None of these events caused study suspension.
Start Your Virtual Consultation
What This Means for You
If you value your time, your mobility, and your independence, the data from this 302-patient trial offers a clear message: biology outperforms synthetic lubrication when it comes to long-term joint preservation.
While this specific study paired the biological injection with an arthroscopic clean-out, the comparative data isolates the profound impact of the adipose tissue itself. When pitted directly against standard HA gel injections, the patient’s own fat tissue proved to be the decisive factor in reducing pain, restoring function, and protecting the joint architecture over a two-year period.
A ~53% improvement in physical function is the difference between sitting on the sidelines and actively participating in your life. It means having the confidence to book a hiking trip, knowing your knees can handle the descent. It means playing a full match on the courts without paying for it with days of throbbing pain afterward. It is about closing the gap between temporary fixes and major surgery.
The MFAT group improved early and did not fade. On multiple symptom scales, benefits stayed meaningfully improved through 24 months, and the gap versus hyaluronic acid was still present at the two-year mark.There was even significant structural improvement seen on MRI.
This research examined micro-fragmented adipose tissue (MFAT), a treatment that shares foundational similarities with Regenerative Matrix Therapy™, RMIC’s next-generation biologic treatment.
By utilizing your body’s biology, we aim to deliver these profound biological benefits directly, helping you reclaim your movement and avoid the downtime of invasive surgery.
Start Your Virtual Consultation
Research Highlights (For Clinicians)
Study Citation: Wu CZ, Shi ZY, Wu Z, et al. Mid-term outcomes of microfragmented adipose tissue plus arthroscopic surgery for knee osteoarthritis: A randomized, active-control, multicenter clinical trial. World J Stem Cells.2023;15(12):1063–1076. doi:10.4252/wjsc.v15.i12.1063.
Study Design: Prospective randomized, active-control, multicenter, single-blind observer trial; 10 hospitals; 24-month follow-up; intention-to-treat with last observation carried forward; repeated-measures analyses with Bonferroni post-hoc comparisons.
Population: Adults aged 30–80 with KL grade 2–3 knee osteoarthritis and symptoms >6 months; 302 randomized. The MFAT group possessed a higher proportion of KL Grade 3 patients at baseline compared to the HA group.
Intervention: Arthroscopy plus MFAT (Lipogems®) vs arthroscopy plus HA (3 injections, 5 mL monthly).
Primary Outcome: WOMAC total at 24 months.
Effect Sizes at 24 Months:
- WOMAC total: ~53% improvement (48.3 → 22.8) vs ~32% (46.5 → 31.7); p < 0.001
- WOMAC pain: ~59% improvement (9.8 → 4.0) vs ~38% (9.5 → 5.9); p < 0.001
- WOMAC stiffness: ~50% improvement (3.2 → 1.6) vs ~33% (3.3 → 2.2); p < 0.001
- WOMAC function: ~51% improvement (35.3 → 17.2) vs ~30% (33.8 → 23.6); p < 0.001
- VAS pain: ~59% improvement (5.3 → 2.2) vs ~48% (5.2 → 2.7); p = 0.006
- Lequesne index: ~33% improvement (10.7 → 7.2) vs ~20% (10.3 → 8.2); p = 0.004
MRI / WORMS:
- MFAT within-group improvement: 58.9 → 55.0; p = 0.020
- HA group: no structural improvement, with a slight trend toward worsening; 60.8 to 62.1; p = 0.850
Safety:
- Serious adverse events: 0% in both groups
- Non-serious effusion/pain/swelling >5 days: 5.4% (8 knees) in MFAT vs 6.2% (9 knees) in control
Limitations:
- Concomitant arthroscopy, so not an injection-only study
- Intention-to-treat with last observation carried forward
- KL grade 2–3 only
Learn More About Regenerative Matrix Therapy™See More Conditions We Treat
Disclaimer
Regenerative Matrix Therapy™ shares foundational similarities with, but is not identical to, the treatment studied. Individual results vary. Educational content only; not a substitute for professional medical advice.
Why Choose Regenerative Matrix Therapy™ With RMIC?
At RMIC, Regenerative Matrix Therapy™ is delivered via a standardized, physician-led protocol built around patient selection, safety, and measurable outcomes. Our adipose-based approach was reviewed by Health Canada with no objection and is designed for patients who do not want to be told to simply “come back when it gets worse.”
If you are exploring advanced, non-surgical options to help manage knee osteoarthritis and preserve your lifestyle, the right next step is a candidacy-focused conversation.