2023 Study: Adipose Therapy and Bone Marrow Equal and Effective in Improving Knee Osteoarthritis
Living in the “Come Back When It’s Worse” Phase
There is a precise, frustrating moment many patients know all too well. You’re sitting in an exam room. The X-rays go up. Your doctor points to the narrowing space in your knee joint—the unmistakable evidence of osteoarthritis. “You have osteoarthritis,” they say. “It’s not severe enough for a total knee replacement yet.” “But it’s too advanced for physiotherapy to fix.”
And then the advice that feels impossible to follow: “Come back when it’s worse.”
For driven individuals—people who built careers, families, and active lives—that “wait until it gets worse” approach feels like surrender. It asks you to accept smaller walks, fewer rounds of golf, skipped ski trips, and hesitation before taking the stairs.
This creates what many describe as a treatment gap: stuck between conservative care and major surgery.
The Biological “Protection Gap” in Knee Osteoarthritis
Knee osteoarthritis is more than just worn-out cartilage. It’s a breakdown of the joint’s biological environment. Healthy joints maintain homeostasis through a complex network of tissues, cells and signaling molecules.
When chronic inflammation sets in, a kind of internal “chemical fire” starts. The challenge is that many conventional options don’t reliably change the trajectory for people who still want to perform:
- Corticosteroids may temporarily suppress inflammation but ultimately causes worsening of the joint condition and speeds up osteoarthritis progression
- Surgery removes the joint entirely and replaces it with metal and plastic implant material
Regenerative approaches such as autologous orthobiologic approaches aim to fill this protection gap by introducing concentrated biologic material from your own body to improve and modulate tissue health to help reduce inflammation. Within the field of regenerative medicine, there is often the question posed of which works better: autologous bone marrow or autologous adipose tissue?
A 2023 prospective comparative clinical trial published in the Journal of Orthopaedic Surgery and Research by Pintore et al. directly examined whether two autologous biologic treatments—bone marrow aspirate concentrate (BMAC) and adipose-derived stem cells (ADSCs)—could meaningfully improve pain and function in symptomatic knee osteoarthritis.
The study included Kellgren–Lawrence (K–L) grades 2–4: 49% K–L Grade 2, 37% K–L Grade 3, and 14% K–L Grade 4 (“bone-on-bone” features). Grade 3–4 generally reflects advanced joint-space narrowing; in grade 4, classic “bone-on-bone” features. This means more than half of participants had moderate to advanced osteoarthritis disease.
Learn More About Regenerative Matrix Therapy™
Study Overview: Adipose vs. Bone Marrow
- Study Design: Prospective comparative clinical trial.
- Participants: 102 patients with symptomatic knee osteoarthritis (Kellgren-Lawrence grades 2–4); 51% with moderate-severe disease.
- The Comparison:
- Group A (n=51): Received Bone Marrow Aspirate Concentrate (BMAC), harvested from the tibia (~10 mL injected intra-articularly).
- Group B (n=51): Received Adipose-Derived Stem Cells (ADSCs), harvested via minimally invasive lipoaspiration and mechanically processed (~10 mL injected intra-articularly).
- Follow-Up Duration: Patients were monitored for 6 months.
- Primary Goals: To assess improvements in pain (VAS), function (KOOS, OKS), and daily living activities, and to directly compare the efficacy of fat-derived vs. bone marrow-derived treatments.
Key Findings: Meaningful Improvement at 6 Months
Across all patients, outcomes improved significantly at 6 months.
1. Pain Was Cut Roughly in Half
The primary driver for seeking treatment is almost always pain—the kind that wakes you up at night or stops you from walking the back nine. In this study, patients treated with adipose therapy saw dramatic reductions in pain scores.
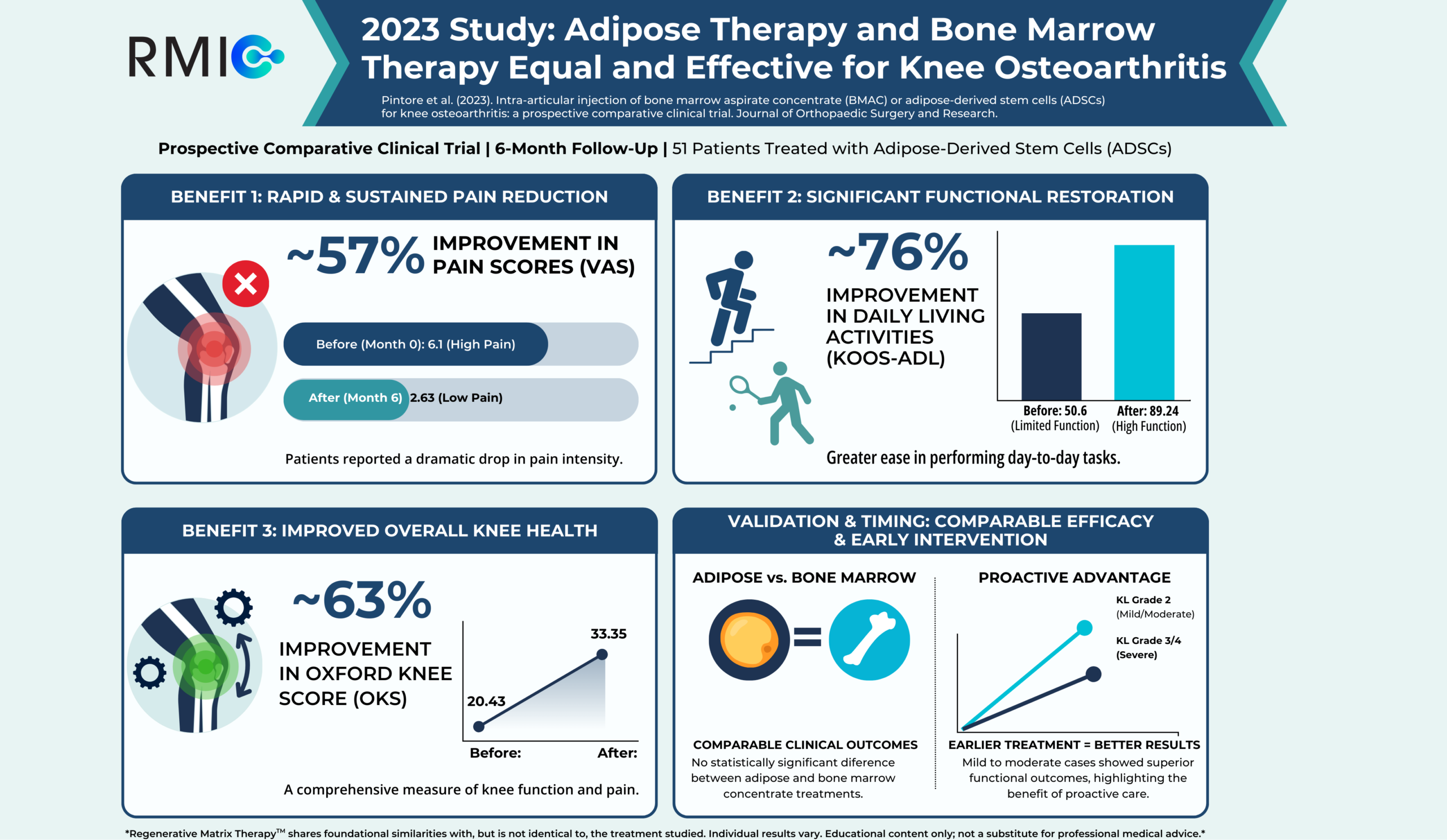
- Visual Analog Scale (VAS) Pain: Participants reported a ~57% reduction in pain (VAS 6.1→ 2.63; p < 0.0001).
- KOOS Pain Score improved dramatically: KOOS pain score more than doubled, indicating a massive improvement in comfort (Score improved from 44.23 → 95.91; p < 0.0001). Note: On the KOOS scale, a higher number indicates less pain/better condition.
For many patients, this type of drastic improvement represents the difference between daily limitation and functional participation.
2. Function and Daily Living Improved Substantially
Pain relief matters—but function means freedom. Patients treated with adipose therapy had a drastic improvement in their daily function.
- Activities of Daily Living (ADL): Patients saw a ~76% improvement in their ability to function day-to-day (Score improved from 50.6 → 89.24; p < 0.0001).
- Oxford Knee Score (OKS): This metric, often used to assess the need for joint replacement, improved by ~63% (Score increased from 20.43 → 33.35; p < 0.0001).
- Quality of life improved ~152% (26.74 → 67.40; p < 0.0001).
These changes reflect patients navigating stairs, getting in and out of cars, and moving through daily life with significantly greater ease; returning to the lives they care about.
3. Adipose and Bone Marrow Showed Comparable Efficacy
When comparing the two most common regenerative medicine treatments for osteoarthritis, bone marrow and adipose, at 6 months, most outcomes were similar.
- No statistically significant difference in VAS at 6 months (p = 0.34).
- Higher OKS at 6 months with BMAC ~83% (20.53 → 37.57) vs ADSCs ~63% (20.43 → 33.35) (p = 0.04), but both groups improved significantly.
- At 1 month, ADSCs showed faster early pain reduction (~70% vs ~49% with BMAC; p < 0.0001).
The critical takeaway: both adipose-derived cells and bone marrow concentrate produced meaningful clinical improvements, with no statistically significant differences between them. While treatment with adipose led to faster and earlier symptom improvement, both groups (bone marrow and adipose) achieved excellent results.
4. Earlier Treatment Produced Better Results
Patients with milder OA (K–L 2) demonstrated statistically superior outcomes compared to K–L 3–4 (p < 0.0001). However, even patients with the most severe Grade 4 (“bone-on-bone”) osteoarthritis still achieved ~45% reduction in pain (VAS 6.2 → 3.4)
Pain reduction at 6 months showed a severity gradient:
- ~62% (VAS 6.7 → 2.53) in K–L Grade 2
- ~48% (VAS 6.78 → 3.53) in K–L Grade 3
- ~45% (VAS 6.2 → 3.4) in K–L Grade 4
Intervening earlier—when the disease is less advanced—was linked to better outcomes, though even those with severe disease still saw significant improvements. This highlights the value of addressing joint issues proactively: starting treatment before major degeneration gives the best chance to maintain function and quality of life. Still, the findings also suggest that improvement is often possible even in later stages.
5. Safety
No complications were reported during follow-up in all 102 patients, demonstrating a perfect safety record in this clinical trial.
Start Your Virtual Consultation
What This Means for You
A single, same-day autologous injection of adipose or bone marrow was associated with significant improvements in pain, daily function and quality of life within 6 months.
A ~57% drop in pain combined with a ~76% improvement in daily function, and a ~152% quality of life improvement is the difference between shrinking your life and reclaiming it.
Furthermore, the equivalence of adipose-based therapy and bone marrow-based therapy validates the concept that both of these regenerative medicine procedures can be powerful tools in treating disease directly at the source, without surgery or just masking symptoms.
If you have moderate-to-severe osteoarthritis, this study suggests improvement is still possible—but the average outcome trends higher in milder disease. That isn’t discouraging; it reinforces the importance of proactive evaluation and personalized candidacy assessment.
This research examined intra-articular BMAC and ADSCs injections, the latter of which shares foundational similarities with (but is not identical to) Regenerative Matrix Therapy™, RMIC’s next-generation adipose-based biologic treatment. Our protocol has been reviewed by Health Canada without objection and is delivered in our licensed clinics across Canada.
The broader message is that biologics may meaningfully delay surgery—and potentially preserve your lifestyle longer. If your goal is to avoid or postpone knee replacement, maintain mobility, and make a science-forward decision based on your imaging and symptoms, start your virtual consultation to see if you’re a candidate.
Start Your Virtual Consultation
Research Highlights (For Clinicians)
Study: Pintore A, Notarfrancesco D, Zara A, et al. Intra-articular injection of bone marrow aspirate concentrate (BMAC) or adipose-derived stem cells (ADSCs) for knee osteoarthritis: a prospective comparative clinical trial. J Orthop Surg Res. 2023;18:350.
Design: Prospective comparative clinical trial; n = 102 (51 BMAC, 51 ADSCs).
Severity: K–L 2/3/4 = 50/38/14 (~14% grade IV).
Follow-Up: 1 and 6 months.
Endpoints: VAS, KOOS (Pain, ADL, QOL), OKS.
Effect Sizes (6 months, overall): VAS ↓ ~54% (6.14 → 2.80; p < 0.0001), OKS ↑ ~73% (20.5 → 35.46; p < 0.0001), KOOS Pain ↑ ~109% (45.37 → 94.76; p < 0.0001)
Between-Group: No significant VAS difference at 6 months (p = 0.34).
Safety: No complications observed.
Limitations: Non-randomized allocation; short follow-up; patient-reported outcomes only; no imaging/cartilage assessment.
Learn More About Regenerative Matrix Therapy™See More Conditions We Treat
Disclaimer
Regenerative Matrix Therapy™ shares foundational similarities with, but is not identical to, the treatment studied. Individual results vary. Educational content only; not a substitute for professional medical advice.
Why Choose Regenerative Matrix Therapy™ With RMIC?
RMIC was built for people who refuse to let knee osteoarthritis quietly shrink their lives. Regenerative Matrix Therapy™ is delivered under a standardized, physician-led protocol focused on safety, candidacy precision, and measurable outcomes.
If you’re exploring non-surgical options to manage knee osteoarthritis and preserve your lifestyle, find out whether Regenerative Matrix Therapy™ may be appropriate for you.